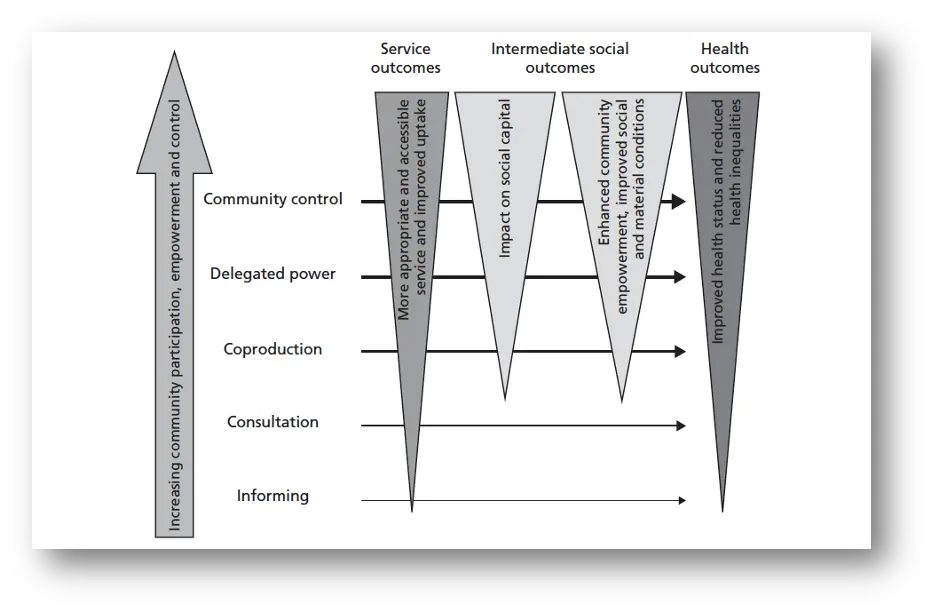
There are numerous models linking community engagement to health improvement. The one we started from was first published in 2006 by Jennifer Popay, now a distinguished professor of sociology and public health at Lancaster University in the UK. I described Popay’s model in post one but the key thing to know is that it incorporates a theory of change that is supported by the research that we reviewed — that the type of outcomes possible depend on the depth of the engagement.
Classically, when the health sector engages communities, it’s either informing its members of something or consulting with them to get their views, perhaps on a health improvement initiative. At that level of engagement, only service outcomes and health outcomes are likely, and they’re usually modest (as indicated by the width of the relevant triangles at those points).
As the engagement deepens, such that community members are involved, collaborated with, or deferred to, ‘community outcomes’ begin to surface. Popay called these ‘intermediate outcomes’, the idea being that they were intermediaries to better service and health outcomes. We’ve called them ‘community outcomes’ because we think they matter in and of themselves, not just because they’re intermediaries to the outcomes that the health sector is classically interested in.
The community outcomes are prerequisites to a community having power. While it’s not inconceivable that they might use that power to improve the health services available to them, as well as their health, it’s also likely that they’ll want to address other things in their neighborhood. Quite what those things are will differ from neighborhood to neighborhood so we’ve depicted it by saying that a community with power has the potential to hold policymakers and institutions accountable.